I was looking at my bibliography from earlier in the year, to see if there was anything that might be useful, and the first source I saw was http://www.bls.gov/oco/ocos294.htm. This is a site from the US Bureau of Labor Statistics. It's all about Athletic Trainers, so I figured it couldn't hurt to look at it and see what they had to say. This is what I found.
Nature
Athletic Trainers prevent and treat injuries for people of all ages. They work with anybody from athletes to industrial workers. They specialize in the prevention, diagnosis, assessment, treatment and rehabilitation of muscle and bone injuries and illnesses. They are the first responding when there is an injury and as such, must be able to recognize, evaluate and assess injuries and provide immediate care when needed.
Athletic Trainers help prevent injuries by educating people on how to reduce their risk of injuries by advising them on proper use of equipment, proper stretching and home exercises. They also help by applying braces or taping athletes to make them more stable.
What Athletic Trainers do is mainly determined by who they are hired. Most Athletic Trainers are hired by a physician, so many spend their time indoors working 40-50 hours per week. However, some Athletic Trainers work as many as 12 hours per day or more, depending on what they do. It is possible, if the trainer works with a collegiate or professional sport that they spend as many as 14 hours per day working.
Qualifications
A Bachelors' degree is usually the minimum degree required to be an Athletic Trainer. However, many Athletic Trainers hold a Masters' or Doctorates' degree. In 2009, 47 states required Athletic Trainers to be licensed. In 2009, there were about 350 accredited collegiate programs in the country. According to the NATA (National Athletic Trainers Association), about 70 percent of Athletic Trainers have at least a Masters' degree.
In order to be certified, one has to take a Board of Certification exam, which is a very rigorous test. The 4 places where certification is not needed (but may prove helpful) are Washington D.C., Alaska, California and West Virginia.
Because of the fact that Athletic Trainers deal not only with athletes, but a variety of people, they should have good communication and people skills. They should be able to manage difficult situations and the stress that comes with them. They should be organized (we'll have to work on that part), have good time management (haha), be inquisitive and have a strong desire to help people. (hey, half ain't bad)
Employment
In 2008, Athletic Trainers held 16,300 jobs all over the country. While most jobs are related to sports, a growing number are not. Many are now found in settings like office buildings, industrial factories, etc. About 39 percent were found in public and private educational services-primarily in high school and college settings. Another 38 percent worked in health care in jobs in hospitals and offices of physicians or practitioners. About 13 percent worked in fitness and recreational sports centers. Lastly, about 5 percent worked in spectator sports.
(Note. This does not add up to 100 percent)
Job Outlook
Employment for Athletic Trainers is projected to increase 37 percent from 2008 to 2018. This is higher than the average for all occupations. This is because of their role in injury prevention and decreasing the cost of health care. Jobs in school settings will be available, but there will be competition in areas like college or spectator sports.
Job growth will be centered in the health care industry, like in hospitals or physicians offices. However, growth in college teams or sports teams will be slower because most already have a complete Athletic Training staff.
As the population ages, it is expected that more elderly people will be turning to Athletic Trainers because they can help to decrease the cost of health care. In some states, there is an effort to have a licensed Athletic Trainer on hand to work with student athletes, so that will open some jobs as well.
Some trainers will be called upon to work in more work-related places to cut down on the costs of health care to the owner. For instance, they may be hired to increase the fitness and performance of policemen and firefighters.
Earnings
Most Athletic Trainers work full time and receive benefits. The salary of an Athletic Trainer depends on experience and job responsibilities. In May of 2008, the median wage for an Athletic Trainer was $39,640. The middle 50 percent earned between $32,070 and $49,250. The lowest 10 percent earned less than $23,450 while the highest 10 percent earned above $60,960.
Showing posts with label Research. Show all posts
Showing posts with label Research. Show all posts
Saturday, June 5, 2010
Tuesday, June 1, 2010
Concussions.....
The bane of the high school athlete...concussions. High schoolers are the most prone to getting a concussion. This is because their brain and skull aren't fully developed, yet they are going at everything 100%, or more in some cases. Younger athletes don't push themselves as hard, and thus aren't as likely to get a concussion as an older athlete. At the same point in time, adult athletes have a fully developed skeletal system, so are less likely to sustain injury to the brain.
A concussion is a traumatic head injury that occurs both from mild and severe blows to the head. It is typically caused by a severe blow during which the brain moves around violently in the skull. Brain cells will fire all at once, much like a seizure. This may result from a fall or when an object hits the head. A sudden turning of the head, like from a punch will more often result in unconsciousness.
Symptoms
Some early symptoms of concussions include
A concussion is a traumatic head injury that occurs both from mild and severe blows to the head. It is typically caused by a severe blow during which the brain moves around violently in the skull. Brain cells will fire all at once, much like a seizure. This may result from a fall or when an object hits the head. A sudden turning of the head, like from a punch will more often result in unconsciousness.
Symptoms
Some early symptoms of concussions include
- Confusion
- Disorientation
- Memory Loss
- Unconsciousness
- Unequally sized pupils
- Headache
- Dizziness
- Tinnitus
- Nausea
- Vomiting
- Vision Changes
- Memory disturbances
- Poor Concentration
- Irritability
- Sleep disturbances
- Personality changes
- Fatigue
Monday, May 31, 2010
Chrondomalacia Patella
Commonly called "Runner's Knee", Chronomalacia Patella is often the cause of pain in the knee. It is common in any sport that involves a lot of running, i.e. cross-country, track, lacrosse, etc. It usually affects healthy, young athletes.
Runner's Knee is caused by an irritation on the underside of the knee. The underside of the patella is covered in a layer of cartilage. The patella can usually glide along with the movement of the knee. However, in some individuals, the patella tends to rub against one side of the knee joint or the other, causing an irritation to the cartilage, thus giving the athlete pain.
Unlike the damage done to the cartilage in arthritis, it is thought that the cartilage from runner's knee can be repaired, because unlike arthritis, it isn't a degeneration of cartilage, it is the blistering that causes the pain.
Along with athletes, women are more likely to get runner's knee than men. It isn't known why, but it's suspected that because of anatomical differences between men and women, there is more lateral force put on the woman's knee than the man's.
Treatment
Most people can get throuh runner's knee if they just rest and do some physical therapy. Letting the inflammation settle is the first part, along with avoiding any activity that would involve heavy stress on the knee, like running or other sports. Gradually the athlete can return to activity. During the time of rest, the athlete can still do cross-training like swimming to keep them active. They can do what they want, as long as it isn't putting a lot of stress on the knee.
Surgery isn't as common as a treatment for runner's knee as it used to be, but it is still used. Sometimes, common therapy is not effective in reducing the inflammation or pain associated with runner's knee, so surgery is necessary.
Runner's Knee is caused by an irritation on the underside of the knee. The underside of the patella is covered in a layer of cartilage. The patella can usually glide along with the movement of the knee. However, in some individuals, the patella tends to rub against one side of the knee joint or the other, causing an irritation to the cartilage, thus giving the athlete pain.
Unlike the damage done to the cartilage in arthritis, it is thought that the cartilage from runner's knee can be repaired, because unlike arthritis, it isn't a degeneration of cartilage, it is the blistering that causes the pain.
Along with athletes, women are more likely to get runner's knee than men. It isn't known why, but it's suspected that because of anatomical differences between men and women, there is more lateral force put on the woman's knee than the man's.
Treatment
Most people can get throuh runner's knee if they just rest and do some physical therapy. Letting the inflammation settle is the first part, along with avoiding any activity that would involve heavy stress on the knee, like running or other sports. Gradually the athlete can return to activity. During the time of rest, the athlete can still do cross-training like swimming to keep them active. They can do what they want, as long as it isn't putting a lot of stress on the knee.
Surgery isn't as common as a treatment for runner's knee as it used to be, but it is still used. Sometimes, common therapy is not effective in reducing the inflammation or pain associated with runner's knee, so surgery is necessary.
Wednesday, May 19, 2010
Torn Rotator Cuff
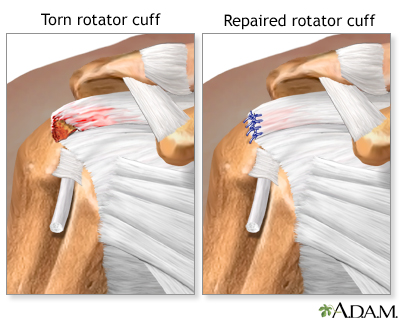
The rotator cuff is a group of muscles and tendons that help to stabilize the shoulder. One or more tendons may become inflamed due to overuse, age, falling or collision. Sports requiring extensive, repeated use of the shoulder have more injuries to the rotator cuff. The injury most often happens to pitchers and quarterbacks because they throw the ball countless times not only during the game but during the week as well.
Signs
Somebody who has an injury to their rotator cuff will likely complain of pain in their deltoid muscle and outer shoulder, especially when the arm is raised in front of them, or out to the side. The shoulder may feel weak, especially when trying to lift the arm into a horizontal position. The athlete may hear a clicking or popping sound in their shoulder when it moves.
How is it diagnosed?
Pain or weakness on an inward or outward rotation of the arm may indicate a torn rotator cuff. There may also be pain when the arm is lowered to the side after the shoulder is moved back and the arm is raised. The problem is that with torn rotator cuffs, you can't look at an X-ray and tell. The shoulder may appear normal. In order to fully detect a torn rotator cuff, an MRI needs to be done, but even that does not detect partial tears.
Treatment
If bad enough, Tommy John surgery may need to be done. However, most times, it is possible to get away with putting heat and ice on teh shoulder and wearing it in a sling for a few days. Other treatments may be done like electrical stimulation, ultrasound or cortisone shots.
On a semi-side note, Tommy John surgery is named after the baseball pitcher, Tommy John, who was the first pitcher to have surgery done to repair his torn rotator cuff. He had 288 victories, the most for any pitcher not selected for the Hall of Fame. He has the 7th highest number of wins for any left-handed pitcher. He made his major league debut for the Cleveland Indians in 1963 and went on to play for the Chicago White Sox, Los Angeles Dodgers, New York Yankees, California Angels, Oakland Athletics and back to the Yankees before he retired in 1989. He had surgery on September 25, 1974.
Monday, May 10, 2010
Achilles Tendonitis
The Achilles Tendon is the most vulnerable tendon in the whole body. It joins the gastrocnemius (calf) and soleus muscles. Tendons are strong, but they aren't very flexible, so they can only go so far before they get inflamed or they tear.
Achilles tendonitis is a chronic injury that comes primarily from overuse. It tends to come on gradually, until it gets to the point that it is too painful to do sports, or even normal daily activities like walking, or getting in the car. The biggest cause of chronic Achilles Tendonitis is ignoring the early signs and pushing through the pain. Another major case is weak calf muscles. If the muscle is weak, it becomes fatigued and it will tighten and shorten. The tightness will increase the stress on the Achilles, and tendonitis can occur. Sudden increases in training, hill climbing, or a lot of speedwork can also lead to Achilles Tendonitis.
At the first sign of pain from the Achilles, the athlete should cut back. Stop speed training, hill running, etc. Begin gentle calf stretching after exercise when the tendon is still warm and flexible, and put ice on the ankle after workouts. Be careful though, not to overstretch. Strengthening the muscle leads to less stress placed on the tendon. Cross-training can also be done while reducing the amount of work done every day. Toe raising, balancing on the toes and wall stretching can also be beneficial.
Achilles tendonitis is a chronic injury that comes primarily from overuse. It tends to come on gradually, until it gets to the point that it is too painful to do sports, or even normal daily activities like walking, or getting in the car. The biggest cause of chronic Achilles Tendonitis is ignoring the early signs and pushing through the pain. Another major case is weak calf muscles. If the muscle is weak, it becomes fatigued and it will tighten and shorten. The tightness will increase the stress on the Achilles, and tendonitis can occur. Sudden increases in training, hill climbing, or a lot of speedwork can also lead to Achilles Tendonitis.
At the first sign of pain from the Achilles, the athlete should cut back. Stop speed training, hill running, etc. Begin gentle calf stretching after exercise when the tendon is still warm and flexible, and put ice on the ankle after workouts. Be careful though, not to overstretch. Strengthening the muscle leads to less stress placed on the tendon. Cross-training can also be done while reducing the amount of work done every day. Toe raising, balancing on the toes and wall stretching can also be beneficial.
Wednesday, May 5, 2010
When The Job's A Game: Athletes, Coaches, Sports Officials and Related Workers
This was a periodical from SIRS Knowledge Source that I found for my bibliography during the first semester. I thought it would be a good idea to look through some of those, so that I had a variety of posts; not just posts about mentor meetings or what I was doing with Kim. This is what it was about.
First of all, it gave an inside look at how all of the different people involved with sports work together. That, I thought, was a really nice touch. It showed how everybody has a major part.
Athlete
During the section specifically about athletes, it talked about how they not only play the game for spectators, but they spend hours and hours under the supervision of coaches and other sports officials while they practice. "To succeed, professional athletes need to understand the rules and strategies of their sport, be in exceptional physical condition, use excellent form and technique, and compete fairly. "
Coaches
Coaches train the athletes by having them perform drills routinely. They improve skills, techniques, conditioning and they strengthen weaknesses. They advise the athletes so that they play to their potential. One of the most important functions of a coach that is often overlooked is the fact that they motivate the athletes to play well. Coaches also instruct their athletes during a game to get the to play the way they need to, or run a certain play, etc.
Sports Officials
This group includes Referees, Umpires and other sports officials. These are the people who control the game. They make sure everything is played according to the rules. They make calls for scoring, outs, just about everything. They promote fair, safe play, and encourage sportsmanship.
Athletic Trainers
They specialize in the prevention, treatment, and rehabilitation of athletic injuries. There are many injuries in the professional sports scene, so they have been necessary there for quite some time. There are still quite a few in college, so many colleges have their own team. More and more high schools have been employing Athletic Trainers to help with student athletes. They help athletes avoid being hurt by teaching them how to condition correctly. Trainers design and monitor strength, cardiovascular and training programs for athletes. Athletic Trainers also select equipment, maintain athletic training areas, stock supplies and keep records.
Scouts
The scouts are there as intelligence agents for the team. They go around looking not only at younger players making their way up, they also look in on other teams to see what they are doing. This helps the team get a better feel for what to expect when they play other teams.
For everybody involved with a job in sports, the hours are very irregular. Some teams have 4-7 month seasons, so many people work part time, and nights and weekends. A trainer for instance will work with the team, not only during the season, but will work with the athletes during the off season so that they stay in shape and continue doing a proper exercise program. During the season, they work with the team, and they travel with the team, so they work many nights and weekends.
Travel is a big part of the job. Half of the games in a professional sport are away from home. In extreme cases, like baseball, that's 81 games away from home. That is a long time, there are stretches where people won't be home for 2-3 weeks at a time, multiple times during the season. It is a big commitment to be involved with a job that is in the sports field.
Kasper, Henry. "When The Job's A Game: Athletes, Coaches, Sports Officials and Related Workers." SIRS Knowledge Source. Gale, Spring 2001. Web. 29 Jan. 2010.
First of all, it gave an inside look at how all of the different people involved with sports work together. That, I thought, was a really nice touch. It showed how everybody has a major part.
Athlete
During the section specifically about athletes, it talked about how they not only play the game for spectators, but they spend hours and hours under the supervision of coaches and other sports officials while they practice. "To succeed, professional athletes need to understand the rules and strategies of their sport, be in exceptional physical condition, use excellent form and technique, and compete fairly. "
Coaches
Coaches train the athletes by having them perform drills routinely. They improve skills, techniques, conditioning and they strengthen weaknesses. They advise the athletes so that they play to their potential. One of the most important functions of a coach that is often overlooked is the fact that they motivate the athletes to play well. Coaches also instruct their athletes during a game to get the to play the way they need to, or run a certain play, etc.
Sports Officials
This group includes Referees, Umpires and other sports officials. These are the people who control the game. They make sure everything is played according to the rules. They make calls for scoring, outs, just about everything. They promote fair, safe play, and encourage sportsmanship.
Athletic Trainers
They specialize in the prevention, treatment, and rehabilitation of athletic injuries. There are many injuries in the professional sports scene, so they have been necessary there for quite some time. There are still quite a few in college, so many colleges have their own team. More and more high schools have been employing Athletic Trainers to help with student athletes. They help athletes avoid being hurt by teaching them how to condition correctly. Trainers design and monitor strength, cardiovascular and training programs for athletes. Athletic Trainers also select equipment, maintain athletic training areas, stock supplies and keep records.
Scouts
The scouts are there as intelligence agents for the team. They go around looking not only at younger players making their way up, they also look in on other teams to see what they are doing. This helps the team get a better feel for what to expect when they play other teams.
For everybody involved with a job in sports, the hours are very irregular. Some teams have 4-7 month seasons, so many people work part time, and nights and weekends. A trainer for instance will work with the team, not only during the season, but will work with the athletes during the off season so that they stay in shape and continue doing a proper exercise program. During the season, they work with the team, and they travel with the team, so they work many nights and weekends.
Travel is a big part of the job. Half of the games in a professional sport are away from home. In extreme cases, like baseball, that's 81 games away from home. That is a long time, there are stretches where people won't be home for 2-3 weeks at a time, multiple times during the season. It is a big commitment to be involved with a job that is in the sports field.
Kasper, Henry. "When The Job's A Game: Athletes, Coaches, Sports Officials and Related Workers." SIRS Knowledge Source. Gale, Spring 2001. Web. 29 Jan. 2010.
Thursday, April 29, 2010
The BOC Exam...
In order to be licensed as an Athletic Trainer, you have to take the Board of Certification exam. It is a very rigorous exam, or so I'm told. In order to be eligible to take the exam you have to meet the following requirements:
Which modality would BEST control pain in a two-day-old Grade I (mild) lateral ankle sprain in a 25-year-old male with Raynaud’s phenomenon? Choose only one.
(Continuous 3 MHz ultrasound should have a bubble by it as well.)
ECC Certification includes:
I found all of this information at http://www.bocatc.org/index.php?option=com_content&view=article&id=10&Itemid=8
- Endorsement of the exam application by the recognized Program Director of the CAATE (Commission on Accreditation of Athletic Training Education) accredited education program
- Proof of current certification in Emergency Cardiac Care (ECC) or proof of enrollment in an approved ECC course
Which modality would BEST control pain in a two-day-old Grade I (mild) lateral ankle sprain in a 25-year-old male with Raynaud’s phenomenon? Choose only one.
(Continuous 3 MHz ultrasound should have a bubble by it as well.)
ECC Certification includes:
- Adult and Pediatric CPR
- AED (Automated External Defibrillator)
- 2nd rescuer CPR
- Airway obstruction
- Barrier devices (e.g., pocket mask, big valve mask, etc.)
I found all of this information at http://www.bocatc.org/index.php?option=com_content&view=article&id=10&Itemid=8
Friday, April 23, 2010
Injuries and Statistics
According to the U.S. Consumer Product Safety Commission Report, sports injuries in baby boomers increased by 31 percent from 1991 to 1998. About 276,000 emergency room cases were for people aged 35-54 in 1991. In 1998, that number skyrocketed to 365,000. In 2006, the NEISS (National Electronic Injury Surveillance System) reported over half a million injuries associated with basketball alone.
Baby boomers suffered over 1 million sports related injuries, which ended up costing $18.7 billion in medical costs in 1998.
Basketball is the sport with the highest number of injuries. I didn't realize there weren't hat many injuries associated basketball. It makes sense though, between the colliding and the jumping involved with basketball, there is a high possibility of injury. One might think that football and lacrosse and other contact sports would be right up there. They are, but you have to remember when thinking about this issue, that with lacrosse, football, etc. the players are wearing pads. In basketball, they aren't.
I've looked, but I couldn't find any statistics about rugby. On this website rugby is combined with lacrosse, and they had relatively few injuries, but I think that that would be a sport that is pretty high as well. There is all of the intense contact of soccer and football, all the collisions, but no padding like in football. I guess I'll just always wonder.
NEISS put out predictions based on 2006 data. Here is what they said
bold=sport
italics=number of projected injuries
Basketball-529,837 These injuries are mainly cut hands, sprained ankles, broken legs, eye and forehead injuries
Bicycling-490,434 These injuries are mainly feet caught in spokes, head injuries from falls, slipping while carrying bicycles, collisions with cars
Football-460,210 These injuries are mainly fractured wrists, chipped teeth, neck strains, head lacerations, dislocated hips and jammed fingers
ATV's, Mopeds, Minibikes-257,123 Riders of ATV's were injured when they thrown. Along with this there were also fractured wrists, dislocated hands, shoulder sprains, head cuts and lumbar strains
Baseball, Softball-274,867 These injuries were mainly head injuries from bats and balls or ankle injuries from running bases or sliding into them
Exercise, Exercise Equipment-269,249 These injuries were mainly twisted ankles and cut chins from tripping on treadmills. Head injuries from falling backward from exercise balls, ankle sprains from jumping rope
Soccer-196,544 This injuries were mainly twisted ankles or knees after falls, fractured arms during games
Swimming-164,607 The injuries were mainly head injuries from hitting the bottom of pools, and leg injuries from accidentally falling into pools
Skiing, Snowboarding-96,119 These injuries were mainly head injuries from falling, cut legs and faces, sprained knees or shoulders
Lacrosse, Rugby-85,580 These injuries were mainly head and facial cuts from getting hit by balls and sticks, injured ankles from falls
This is a comparison of injuries associated with 16 popular sports between 1991 and 1998.

http://www.scientificpsychic.com/fitness/sport_injuries.html
Baby boomers suffered over 1 million sports related injuries, which ended up costing $18.7 billion in medical costs in 1998.
Basketball is the sport with the highest number of injuries. I didn't realize there weren't hat many injuries associated basketball. It makes sense though, between the colliding and the jumping involved with basketball, there is a high possibility of injury. One might think that football and lacrosse and other contact sports would be right up there. They are, but you have to remember when thinking about this issue, that with lacrosse, football, etc. the players are wearing pads. In basketball, they aren't.
I've looked, but I couldn't find any statistics about rugby. On this website rugby is combined with lacrosse, and they had relatively few injuries, but I think that that would be a sport that is pretty high as well. There is all of the intense contact of soccer and football, all the collisions, but no padding like in football. I guess I'll just always wonder.
NEISS put out predictions based on 2006 data. Here is what they said
bold=sport
italics=number of projected injuries
Basketball-529,837 These injuries are mainly cut hands, sprained ankles, broken legs, eye and forehead injuries
Bicycling-490,434 These injuries are mainly feet caught in spokes, head injuries from falls, slipping while carrying bicycles, collisions with cars
Football-460,210 These injuries are mainly fractured wrists, chipped teeth, neck strains, head lacerations, dislocated hips and jammed fingers
ATV's, Mopeds, Minibikes-257,123 Riders of ATV's were injured when they thrown. Along with this there were also fractured wrists, dislocated hands, shoulder sprains, head cuts and lumbar strains
Baseball, Softball-274,867 These injuries were mainly head injuries from bats and balls or ankle injuries from running bases or sliding into them
Exercise, Exercise Equipment-269,249 These injuries were mainly twisted ankles and cut chins from tripping on treadmills. Head injuries from falling backward from exercise balls, ankle sprains from jumping rope
Soccer-196,544 This injuries were mainly twisted ankles or knees after falls, fractured arms during games
Swimming-164,607 The injuries were mainly head injuries from hitting the bottom of pools, and leg injuries from accidentally falling into pools
Skiing, Snowboarding-96,119 These injuries were mainly head injuries from falling, cut legs and faces, sprained knees or shoulders
Lacrosse, Rugby-85,580 These injuries were mainly head and facial cuts from getting hit by balls and sticks, injured ankles from falls
This is a comparison of injuries associated with 16 popular sports between 1991 and 1998.

http://www.scientificpsychic.com/fitness/sport_injuries.html
Tuesday, April 20, 2010
Torn ACL
There are 4 ligaments that stabilize the knee. The four are the MCL, LCL, PCL and ACL. The MCL is the medial collateral ligament; the LCL the lateral collateral ligament. These are the two that run down the sides of your knee, the MCL is on the inside, the LCL the outside. Contrastingly, the PCL is the posterior cruciate ligament and the ACL the anterior cruciate ligament. The PCL runs down the back of the knee, and the ACL runs down the front.
Last year, I sprained my PCL in dance. It is much more difficult to do that than to sprain or tear the ACL. However, it is much more difficult to repair the ACL and to rehab it than it is to work with rehabbing the PCL.
The ACL is crucial to knee stability. It helps to prevent excessive motion. Most people who have torn their ACL will complain of a feeling that their knee is "giving out" from under them.
An ACL tear is usually sports related, but can happen in motor vehicle accidents, falls and work related injuries as well. Approximately 80% of sports related ACL tears are non-contact tears. This means that they don't involve another athlete in the injury. Most of them are from landing from a jump or from pivoting on the leg while running. Interestingly, women are more prone to injury involving the ACL than men are, but it is unclear as to why this is.
Symptoms
People who have a torn ACL often complain of hearing or feeling a pop in their knee at the time of the injury. The loudness of the pop surprises a lot of people; people can usually hear it from the sidelines of a game. Even if you don't hear the pop, you will usually feel the shift in the joint. There are always those people though who have no idea that they've sustained an injury. It has been known that people don't always feel the tear. People have gotten hurt, not realized it, felt fine and continued with the game. It has happened.
Other symptoms include the giving out that was mentioned earlier and swelling and pain in the knee.
Surgery?
People can get surgery done to reconstruct their ACL, however it might not be necessary. If you don't do a sport routinely that requires the use of your knee, and you don't have knee instability, then you probably won't need to have surgery to reconstruct the ACL. There is also a debate over whether to perform surgery on a partial tear. Some say that you can, but others say that it's better not to do it. Most people start feeling better after a few weeks, but problems with instability might continue.
At Ithaca High this year, we've had three ACL tears. Two guys and one girl tore their ACLs this year. One was in soccer, one in football, and one in lacrosse. ACL injuries are also more common in younger people. There is a debate in the health professions about what to do when the ACL injury happens to somebody who is not only younger, but a child. Some people say that it is better to repair the ACL before skeletal maturity, however, the other side says that problems that arise may lead to growth plate closure or alignment deformities. Who knows what's going to happen?
Last year, I sprained my PCL in dance. It is much more difficult to do that than to sprain or tear the ACL. However, it is much more difficult to repair the ACL and to rehab it than it is to work with rehabbing the PCL.
The ACL is crucial to knee stability. It helps to prevent excessive motion. Most people who have torn their ACL will complain of a feeling that their knee is "giving out" from under them.
An ACL tear is usually sports related, but can happen in motor vehicle accidents, falls and work related injuries as well. Approximately 80% of sports related ACL tears are non-contact tears. This means that they don't involve another athlete in the injury. Most of them are from landing from a jump or from pivoting on the leg while running. Interestingly, women are more prone to injury involving the ACL than men are, but it is unclear as to why this is.
Symptoms
People who have a torn ACL often complain of hearing or feeling a pop in their knee at the time of the injury. The loudness of the pop surprises a lot of people; people can usually hear it from the sidelines of a game. Even if you don't hear the pop, you will usually feel the shift in the joint. There are always those people though who have no idea that they've sustained an injury. It has been known that people don't always feel the tear. People have gotten hurt, not realized it, felt fine and continued with the game. It has happened.
Other symptoms include the giving out that was mentioned earlier and swelling and pain in the knee.
Surgery?
People can get surgery done to reconstruct their ACL, however it might not be necessary. If you don't do a sport routinely that requires the use of your knee, and you don't have knee instability, then you probably won't need to have surgery to reconstruct the ACL. There is also a debate over whether to perform surgery on a partial tear. Some say that you can, but others say that it's better not to do it. Most people start feeling better after a few weeks, but problems with instability might continue.
At Ithaca High this year, we've had three ACL tears. Two guys and one girl tore their ACLs this year. One was in soccer, one in football, and one in lacrosse. ACL injuries are also more common in younger people. There is a debate in the health professions about what to do when the ACL injury happens to somebody who is not only younger, but a child. Some people say that it is better to repair the ACL before skeletal maturity, however, the other side says that problems that arise may lead to growth plate closure or alignment deformities. Who knows what's going to happen?
Tuesday, April 6, 2010
Sprained Ankles
Another injury that seemed common on the Lacrosse Injuries Forum was sprained ankles.
Oh, here's the link to that forum if you want it...
http://forums.insidelacrosse.com/showthread.php?t=39299
Anyways, like I said, sprained ankles seemed common among the list of injuries commonly sustained by a lacrosse player.

A sprained ankle, or a twisted ankle, is the stretching or tearing of ligaments. The most common kind of ankle sprain is an inversion sprain. When this happens, the bottom of the foot faces inwards, which damages the ligaments on the outside of the foot.
A medial ligament sprain rarely occurs. This would be when the bottom of the foot is facing outward. When it does occur, it is usually in conjunction with a fracture.
The most common ligament injured in an ankle sprain is the anterior talofibular ligament. This ligament connects the talus (ankle bone) to the smaller bone in the calf, the fibula.
However, if the sprain is severe, there could be damage to
the calcaneofibular ligament which connects the heelbone to
the fibula.
In addition to ligament injuries, tendons, bones, and other tissue might also be damaged. Because of this, it is important to get an x-ray of the ankle if sprained, because small fractures are not uncommon.
With a severely sprained ankle, there can be complete ruptures of the anterior talofibular, calcaneofibular, and posterior talofibular ligaments. These can result in a dislocation of the ankle joint which is often associated with fractures.
There are three stages of ankle sprains.
Stage 1:
Immediate:
RICE
R: Rest. This helps to reduce pain and prevent further damage. Many therapists say to have some moderate weight on the foot as soon as possible-it is thought to accelerate rehabilitation.
I: Ice. Applying ice and compression can reduce pain and swelling and encourage blood flow. Apply an ice pack immediately for 15 minutes and repeat every 2 hours.
C: Compression. This reduces bleeding and swelling.
E: Elevation. Elevation uses gravity to reduce swelling and bleeding by allowing the fluids to flow away from the injury.
Later on, strengthening things such as ankle circles can get the ankle moving again and reduce swelling even more. After a sprain, the calf muscle often tightens up so protect the joint, so slowly strengthening the calf can also help get the rehab done quicker.
Oh, here's the link to that forum if you want it...
http://forums.insidelacrosse.com/showthread.php?t=39299
Anyways, like I said, sprained ankles seemed common among the list of injuries commonly sustained by a lacrosse player.

A sprained ankle, or a twisted ankle, is the stretching or tearing of ligaments. The most common kind of ankle sprain is an inversion sprain. When this happens, the bottom of the foot faces inwards, which damages the ligaments on the outside of the foot.
A medial ligament sprain rarely occurs. This would be when the bottom of the foot is facing outward. When it does occur, it is usually in conjunction with a fracture.
The most common ligament injured in an ankle sprain is the anterior talofibular ligament. This ligament connects the talus (ankle bone) to the smaller bone in the calf, the fibula.
However, if the sprain is severe, there could be damage to
the calcaneofibular ligament which connects the heelbone to
the fibula.
In addition to ligament injuries, tendons, bones, and other tissue might also be damaged. Because of this, it is important to get an x-ray of the ankle if sprained, because small fractures are not uncommon.
With a severely sprained ankle, there can be complete ruptures of the anterior talofibular, calcaneofibular, and posterior talofibular ligaments. These can result in a dislocation of the ankle joint which is often associated with fractures.
There are three stages of ankle sprains.
Stage 1:
- some stretching of the ligaments, possible minor tearing of the lateral ligaments
- little or no joint instability
- mild pain
- mild swelling around the bone on the outside of the ankle
- some joint stiffness while walking or running
- moderate tearing of the ligaments
- some instability of the joint
- moderate to severe pain, and difficulty walking
- swelling and stiffness in the ankle joint
- minor bruising
- total rupture of the ligament(s)
- major instability of the joint
- severe pain initially followed by no pain later
- severe swelling
- extensive bruising
Immediate:
RICE
R: Rest. This helps to reduce pain and prevent further damage. Many therapists say to have some moderate weight on the foot as soon as possible-it is thought to accelerate rehabilitation.
I: Ice. Applying ice and compression can reduce pain and swelling and encourage blood flow. Apply an ice pack immediately for 15 minutes and repeat every 2 hours.
C: Compression. This reduces bleeding and swelling.
E: Elevation. Elevation uses gravity to reduce swelling and bleeding by allowing the fluids to flow away from the injury.
Later on, strengthening things such as ankle circles can get the ankle moving again and reduce swelling even more. After a sprain, the calf muscle often tightens up so protect the joint, so slowly strengthening the calf can also help get the rehab done quicker.
Sunday, March 28, 2010
Shin Splints

I was looking up "Common Lacrosse Injuries" on Google and I came across a link that led me to a forum. This girl was writing a paper for her Athletic Training class and he had to research Common Lacrosse Injuries. So she asked what the most common ones were. I looked over the list and the one that kept coming up was shin splints. So, I figured I would start there.
Shin splints are defined as pain along the front or inside edge of the shinbone (tibia). They are common among athletes who run and jump. Pain along the front of the tibia is called anterior shin splints, while pain along the inside of the tibia is called posterior shin splints.
Shin splints are usually the result of overuse. If an athlete hasn't trained in a while or hasn't done the exact thing that they are asked to do in a while, chances are they are going to get shin splints. Repeated movements of the foot can lead to the tibialis muscles pulling away from the bone. The injured muscle and the bone covering may become inflamed.
Anterior shin splints tend to happen to people who take up a new activity like jogging, sprinting or an activity that requires sudden starting and stopping. Running downhill can lead to and even bigger effect because the muscles in the lower leg have to control the planting of the foot which is more difficult when running downhill. People who run on the balls of their feet or who don't have good running shoes likely have a big problem with anterior shin splints.
Posterior shin splints likely result from imbalances in the leg and foot. Muscle imbalances from a tight calf muscle can lead to this problem. One major cause of posterior shin splints is having flat feet. As the foot flattens out, the posterior tibialis muscle gets stretched and will tug on its connection to the bone. The attachment eventually becomes damaged, leading to irritation; posterior shin splints.
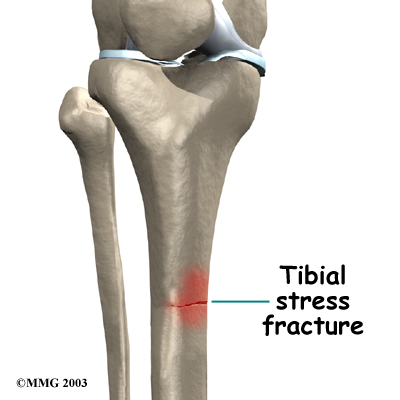
A stress fracture in the tibia can have many of the same symptoms as shin splints, so it can be hard to differentiate between the two. A stress fracture is a crack in a weakened area of the bone. Continual stress from running on hard surfaces or from heavy strain on the muscles can lead to tibial stress fractures. People with shin pain who try to work through it can often develop a stress fracture.
One big issue surrounding shin splints is compartment syndrome. Compartment syndrome is when pressure from muscle damage and swelling builds up in a certain "compartment" of the body. As the pressure builds, the capillaries that bring blood to the area are squeezed shut. When the blood is not getting to the muscle, it can lead to a pain. like a muscle cramp. If the pressure continues to rise, it can lead to coldness, numbness, and swelling in the lower leg and foot. If the pressure builds up and is not treated, it can cause serious tissue damage in the leg and foot.
When someone is experiencing shin splints, they will often feel a dull ache where the muscles attach to the bone. Redness and swelling can also be found in this area. There might be small bumps or ridges along the part of the leg where the person is experiencing pain.
Diagnosis is usually made through physical examination. Reducing inflammation is the first step to fixing shin splints. This can be done with ice, rest, and taping of the shin. Iontophoresis can be used. It is when a small electrical current is used to push a steroid up the leg into the sore area. Ultrasound treatments and deep tissue massage can also be used.
Surgery is rarely needed to help shin splints. However, shin splints where there is also some compartment syndrome might need surgery, sometimes immediately.
Sunday, March 21, 2010
A bit more...
So, I did a bit more research today. This time it wasn't periodicals that I was looking at because I've decided that I am going to use the "Relief in a World of Hurt" article. I did some research on common Lacrosse injuries. I think i am going to need to focus on maybe the upper or lower half of the body because there are so many injuries. I haven't yet decided what part of the body I am going to focus on, I will know that after a bit more research, so until then, I'll leave both you and I wondering. However, when I know, you'll know.
Until tomorrow....
Tuesday, March 16, 2010
Another Mentor Meeting
I met with Mr. Heurich today 7th period. We talked about what I have done this week, and some ideas for new posts that I could write...I have already written a blog about the ideas...look below. We also talked about what my plans are for my presentation.
As far as the presentation goes, I would like to give a taping lesson to people. I don't know if it would be ankle taping, wrist taping, etc, but I think it would be a good idea to look at doing that as a culmination of all the things i've learned about Athletic Training. Along with that, I thought of having some handouts with pictures of injuries, and I could have a someone come in and demonstrate how doing a certain thing could cause the injury, and I could stop them as soon as the injury would occur.
Mr. Heurich and I also talked about doing a blog about the differences between Athletic Training and Physical Therapy. There are a lot of differences, but a lot of people don't know what those differences would be off the top of their head, so it would be a little more information to help peOple understand just what I want to do with my life after high school and college. Even I am not totally sure of all of the differences, so it would help not only the general public that doesn't know about Athletic Training, it would be able to help me as well.
Part of the reason that I wanted to do this project was that I wanted to make sure that the field that I definitely wanted to go into in college was Athletic Training. That's what I love about this project so much. It helped me to officially decide that I want to go into Athletic Training. Yay!!
Mrs. Sauls suggested that I look at a magazine called Oxygen. It is about women and them getting in shape and doing things to help their bodies, and I think this a great idea. I am going to take a look at this magazine at the earliest possible time...which might be in a few days after I have looked at Runner's World, the magazine not the online articles...so we'll see.
I guess that's all for now...bye! :)
Entry Idea
Entry Ideas:
- Write an overview of the kinds of fitness and injury prevention articles found in various popular magazines such as Oxygen, Runner's World, etc.
- Develop the perfect marketing plan for a new magazine that would fit in a niche-for the general public about all different kinds of sports.
- More analysis of taping videos and prevention clips found online.
Friday, March 12, 2010
IC Training Room
I went over to teh Training Room today. I spoke to Chris Hummel. By an extreme amount of good luck, he happens to be the Athletic Trainer for the Ithaca College Gymnastics team. Good luck, right? I told you. So, I asked him questions about what the common injuries were in gymnastics and he gave me a list of five. They are:
That's it for now...
- Tibia Stress Fractures
- Ankle Sprains
- Stress Fractures in the Lumbar Spine (Spondylysis, commonly called "Spondy")
- ACL injuries
- Concussions
- Educating the athletes on the possible injuries and informing them of issues with them, etc.
- Having them come in as soon as possible, if they have any early signs, meet with an Athletic Trainer
- Talking with an Athletic Trainer about the history of their injuries
- Strengthening as far as ankle injuries go
- Mechanics of jumping and landing with an ACL injury
That's it for now...
Wednesday, March 10, 2010
A Little Bit of Research
Today, 7th and 8th periods, I went to the Library and borrowed one of the boxes of magazines that Mr. Heurich and I talked about yesterday, DanceSpirit. It wasn't very helpful, the magazines are more about costumes, competitions and famous dancers and choreographers than it is about injuries and things that I am looking for. However, I had fun looking at it. I recognized some people and some of the costumes that were featured in the magazine. For instance, on the cover of one of the magazines was Maud Arnold. I met her February 20th, in Syracuse, she was my Tap teacher at a competition that I was at. This, for me, was the best part of the whole bit...the fact that I knew her and she was on the cover. It was pretty cool.
I think I'm going to go back and look at Runner's World Magazine to see what I can find in there, if anything. Having the magazines at school is getting me so amped. This way I'm not just looking at the computer screen trying to read periodicals all the time. I think I am going to be doing a lot more work now that I have that resource.
I think I'm going to go back and look at Runner's World Magazine to see what I can find in there, if anything. Having the magazines at school is getting me so amped. This way I'm not just looking at the computer screen trying to read periodicals all the time. I think I am going to be doing a lot more work now that I have that resource.
Tuesday, March 9, 2010
Pain relief for runner's knee from RunnersWorld.com
Pain relief for runner's knee from RunnersWorld.com
I found this website with Mr. Heurich and it shows some cool information about taking care of yourself and preventing injuries like runner's knee if you are a runner. The website is runnersworld.com.
Mentor Meeting 3/9/10
Today is my third meeting with Mr. Heurich. I filled him in on what I have done lately...keeping him apprised of what my progress is.
What I've Done Since Last Meeting
- Met with Kim Bailey for the first time and saw her taping some of the athletes
- Looked up some videos of taping knees and ankles on youtube (will blog about some of the videos that I liked and that were useful)
- Read another periodical online, however it was of no help
- Set up an appointment with Dr. Getzin for the 24th of March to talk to him about my back along with talking about common injuries in sports.
What I plan To Do
- Before the next meeting, I am going to come into the library and look at some magazines that Mr. Heurich and I found. One magazine is DanceSpirit, another is Runner's World to se if they have anything that could be useful to me.
- I am going to meet with Kim Bailey again today and any other day that I can to keep going on my interning. I will talk to her to see if I can find out any more on the common injuries that she works with. I don't know that I will have a lot of time to do this because it is the beginning of the season and she is going to have a lot to do getting ready and getting Impact Testing done. Impact Testing is testing to see if an athlete has a concussion or not to start the season.
- I will blog about any videos that I found useful and interesting from YouTube.
- I am going to work on making my blog media-rich. This will include videos, pictures. Anything that I learn or want to learn will be included from now on.
Wednesday, March 3, 2010
Taping Video
For part of my project, I wanted to learn some basic techniques for taping of all kinds, whether it be ankle, knee, wrist, whatever. In my meeting with Mr. Heurich the other day, we found this video and I watched it in its entirety at home that night and it looked really interesting, and answered a question I had when I went to see Kim last week. I saw her tape an ankle for a basketball player, and I wondered what the things were that she was putting on either side of the ankle, and I didn't have a chance to ask the question, but this video answered that question for me.
If you don't know, a sprain is when the ligaments stretch or tear. An inversion ankle sprain that was mentioned in the video is when the ankle is rolled to the outside thus either stretching or tearing that ligament. The heel lock that he was putting on after the stirrup help to prevent this from happening.
If you don't know, a sprain is when the ligaments stretch or tear. An inversion ankle sprain that was mentioned in the video is when the ankle is rolled to the outside thus either stretching or tearing that ligament. The heel lock that he was putting on after the stirrup help to prevent this from happening.
Thursday, February 25, 2010
Periodicals
I spent part of my day today looking at periodicals that I had put in by Annotated Bibliography. The first one that I read was entitled, "Overuse Injuries in Young Athletes". While the article itself wasn't very helpful, there was a section at the end that talked about recognizing and preventing overuse injuries. I don't know if this will be helpful to me or not in the future, but it might give me a place to start when I talk to people in the future.
The works cited for the article is:
Billhartz Gregorian, Cynthia. "Overuse Injuries Plague Young Athletes." SIRS Knowledge Source. Gale, 11 Jan. 2008. Web. 29 Jan. 2010.
I have been looking over a bunch of other articles that I chose briefly, and they looked to be either as helpful or more helpful than this article was. I hope to be able to blog about those very soon.
The works cited for the article is:
Billhartz Gregorian, Cynthia. "Overuse Injuries Plague Young Athletes." SIRS Knowledge Source. Gale, 11 Jan. 2008. Web. 29 Jan. 2010.
I have been looking over a bunch of other articles that I chose briefly, and they looked to be either as helpful or more helpful than this article was. I hope to be able to blog about those very soon.
Subscribe to:
Posts (Atom)